

Background: Patients with pancreatic cancer have a high risk for venous thromboembolism (VTE). Activation of haemostasis has been suggested to contribute to the progression of cancer and its metastatic spread. However, clinical data to support the contribution of activation of haemostasis to disease progression are scarce. Our aim was to evaluate the association biomarkers indicating activation of haemostasis and/or hypercoagulability and of VTE occurrence with survival and therapy response in patients with pancreatic cancer.
Methods: Within a prospective, observational cohort study (Vienna Cancer and Thrombosis Study, CATS), we evaluated the subgroup of patients with pancreatic cancer (n=145). Levels of a comprehensive panel of haemostatic biomarkers (D-dimer, prothrombin fragment 1+2, fibrinogen, factor VIII, plasminogen activator inhibitor 1 (PAI-1), soluble (s)P-selectin, peak thrombin generation, endogenous thrombin potential) were measured at baseline. Differences in levels of haemostatic biomarkers between disease stages were tested for statistical significance by Kruskal-Wallis-test. The association of biomarker levels with overall survival (OS) and therapy response (progression-free survival (PFS) and radiological disease control rate; sub-cohort of patient initiating palliative chemotherapy, n=95) was analysed by multivariable Cox regression, adjusting for disease stage, grade, sex, age, ECOG, VTE (as time-dependent covariable) and vascular infiltration or compression by the primary tumour. Cumulative incidence of VTE was estimated in competing risk analysis, considering death as competing outcome event. The impact of VTE on OS and PFS was evaluated by multi-state modelling, adjusting for stage, grade, sex, age, ECOG and vascular involvement.
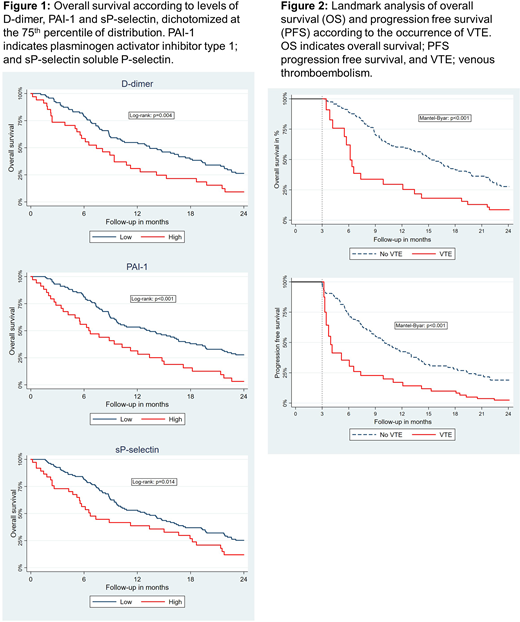
Results: We observed higher baseline levels of biomarkers according to increasing stage of disease for D-dimer (stage I/II: median 1.25 µg/ml [interquartile range (IQR): 0.65-2.10]; stage III: 1.41 µg/ml [IQR: 0.65-2.24]; stage IV: 1.68 µg/ml [IQR: 0.98-3.82], p=0.035), and sP-selectin (stage I/II: median 34.2 ng/ml [IQR: 26.8-43.1]; stage III: 37.6 ng/ml [IQR: 31.4-49.1]; stage IV: 38.8 ng/ml [IQR:32.9-51.5], p=0.033). Higher levels of D-dimer, PAI-1 and sP-selectin were associated with shorter OS in multivariable analysis (hazard ratio (HR) for death per doubling: 1.33 [95% confidence interval (CI): 1.08-1.66], 1.25 [95% CI: 1.08-1.45, and 1.42 [95% CI: 1.00-2.01] (Figure 1). In the subgroup of patients initiating palliative chemotherapy, pre-therapeutic levels of D-dimer predicted for shorter PFS (HR for disease progression per double: 1.29 [95% CI: 1.03-1.61]) and a decreased probability for radiological therapy response (odds ratio to achieve radiological disease control per double: 0.61 [95% CI: 0.38-0.99]). Cumulative incidence estimates of VTE in competing risk analysis at 3, 6, 12, and 24 months were 9.0% [95% CI: 5.0-14.3], 13.1% [95% CI: 8.2-19.1], 16.6% [95% CI: 11.1-23.1], and 19.5% [95% CI: 13.4-26.2], respectively. The occurrence of VTE was associated with an immediate increase in risk of death (transition hazard ratio, (THR): 2.37 [95% CI: 1.47-3.84]) and early disease progression (THR: 2.34 [95% CI: 1.50-3.66]), which prevailed upon multivariable adjustment. In landmark analyses, median OS and PFS after VTE were 5.5 months [95% CI: 2.2-6.5] and 3.0 months [95% CI: 1.5-3.9] compared to 13.4 months [95% CI: 9.7-16.6] and 7.5 months [95% CI: 5.9-9.8] in those without VTE (Mantel-Byar: both p<0.001). Figure 2 displays landmark analyses of OS and PFS according to occurrence of VTE within the first 3 months of observation.
Conclusion: Occurrence of VTE, activation of haemostasis and hypercoagulability, as indicated by elevated levels of D-dimer, PAI-1 and sP-selectin are associated with poor prognosis and D-dimer predicts for unfavourable response to palliative chemotherapy in patients with pancreatic cancer.
No relevant conflicts of interest to declare.

